
According to the data of the Swedish Prosthesis Register system, total hip prosthesis due to arthritis is numerically in front of all other prostheses.
Hip replacement surgery is a treatment for patients who have pain due to arthritis of the hip joint and whose daily activities are restricted. It is based on replacing the upper part of the thigh bone and the nest with artificial joints. It can be metal, polyethylene or ceramic.
Preoperative planning in handmade hip prosthesis is done on 2 dimensional drawings. (1) How to place the parts during surgery depends on the experience of the surgeon. Even in the reliable applications, there is a risk of dislocation, re-operation and delay in the hospital duration. (2-3)
Hip replacement surgery is a treatment for patients who have pain due to arthritis of the hip joint and whose daily activities are restricted. It is based on replacing the upper part of the thigh bone and the nest with artificial joints. It can be metal, polyethylene or ceramic.
Preoperative planning in handmade hip prosthesis is done on 2 dimensional drawings. (1) How to place the parts during surgery depends on the experience of the surgeon. Even in the reliable applications, there is a risk of dislocation, re-operation and delay in the hospital duration. (2-3)
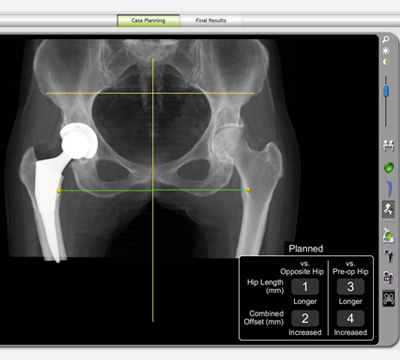
3-dimensional anatomy of the nest can be designed with Makoplasty (Robotic Hip Replacement). Thus, the placement and position of the nest are performed as desired. Immediate changes are monitored and controlled using Haptic technology with sensors. Using these advantages of robotic hip surgery; the most important cause of post-operative dislocation risk, fit of the nest and head is idealized. The risk of inequality related to leg length is eliminated.
Studies have shown that only 47% of the nest placement can be made to the ideal site in handmade prosthesis. It is seen that the nest implants made with Makoplasty are 6 times more accurate angularly than those handmade ones. (4-5-6)

In summary, Makoplasty is a technology that is widely available to use in the hip, and provides accurate positioning of the implant. Minimally invasive can be applied.
Early movement and long implant life are targeted by preserving the soft tissue and mechanical balance of the joint.
REFERENCES
- 1. Hafez M, Jaramaz B, DiGioia III, A. Surgical Treatment of Hip Arthritis: Reconstruction, Replacement and Revision; Chapter 66, October 2009.
- 2. Phillips C, Barret J, Losina E, et al. Incidence of dislocation, pulmonary embolism, and deep infection during the first six months after elective total hip replacement. J Bone Joint Surgery Am. 2003;85:2026.
- 3. Bozic KJ, Kurtz SM, Lau E, Ong K, Vail TP, Berry DJ. The epidemiology of revision total hip arthroplasty in the United States. J Bone Joint Surg Am. 2009;91:128–133.
- 4.Kennedy J, Rogers W, Soffe K, sullivan R, Griffen D, sheehan I. Effect of acetabular component orientation on recurrent dislocation, pelvic osteolysis, polyethylene wear, and component migration. J Arthroplasty. 1998;13:533-534.
- 5.Malik A, Maheshwari A, Dorr L. Impingement with total hip replacement. J Bone Joint Surg Am. 2007;89:1832-1842
- 6.Bozic K, Kurtz S, Lau E, Ong K, Vail T, Berry D. The epidemiology of revision total hip arthroplasty in the United States. J Bone Joint Surg Am. 2009;91:128-133